

Gout is painful inflammatory arthritis, and it is the most common form of inflammatory arthritis. Gout occurs because of the deposition of monosodium urate crystals in the joints. It mostly affects the first metacarpophalangeal joint of the big toe. Gout affects males more than females, and it is uncommon in females before menopause. According to the center for disease control and prevention (CDC), 8.3 million people have gout in the USA between 2007 and 2008. Also, the risk of gout increases among people who suffer from chronic diseases, such as diabetes mellitus, hypertension, obesity, hyperlipidemia, and cardiovascular diseases.
We will discuss gout in more detail, and we will answer the following questions about it:
- What are the causes and risk factors that of gout?
- What is the clinical presentation of gout?
- How can a doctor diagnose gout?
- What is the treatment of gout, either during the attack or between attacks?
- What is the prognosis of gout?
Causes and risk factors of gout


Gout results from increased uric acid in the blood, which leads to the deposition of monosodium urate crystals in the joint or any other tissue. Uric acid is the product of the metabolism of purine proteins (nucleoproteins that contribute to DNA synthesis). Kidneys get rid of the uric acid in the urine and prevent its deposition in the body tissues. But in certain conditions, hyperuricemia may occur due to increased production or decreased excretion of the uric acid.
1) Increased uric acid production may be:
- Primary: It results from a defect in the HGPRT(Hypoxanthine-Guanine-Phosphoribosyl-Transferase) enzyme, which contributes to purine metabolism. This enzyme reduces uric acid production. It converts the hypoxanthine into Inosine monophosphate, which reverses the direction of purine metabolism.
- Secondary: Some medical conditions may increase the purine metabolism and uric acid production, such as leukemia, lymphoma, sarcoidosis, and psoriasis. Also, chemotherapy of leukemia and lymphoma increases the release of uric acid into the blood due to increased purine turnover.
2) Reduced uric acid excretion may be:
- Primary: Idiopathic isolated tubular deficiency
- Secondary:
- Renal failure
- Dehydration -due to decreased renal blood flow-
- Hypothyroidism and hyperparathyroidism
- Acidosis: such as ketoacidosis in diabetes mellitus, lactic acidosis as in alcohol, and starvation
♦ Besides the causes, some risk factors increase the risk of gout, such as:
- Age and gender: Gout is more common in males who are 40 or 50 years old. Before menopause, the risk of gout is low in females, but it increases postmenopausal.
- Positive family history of gout.
- Diet: Purine-rich foods increase the gout risk, such as red meat, organ meat, shrimp, dried mushrooms, dried anchovies, and other seafood like scallops, tuna, and sardines. Also, fructose-rich foods and drinks increase the risk of gout.
- Alcohol: It is one of the most potent risk factors of gout; more alcohol consumption means a higher risk of gout.
- Health problems, such as hypertension, diabetes mellitus, obesity, dyslipidemia, lead poisoning, and heart failure, may increase the risk of getting gout.
- Surgery and trauma
- Infection
- Dehydration and starvation
- Medications: such as diuretics, pyrazinamide, the low dose of aspirin, the high dose of niacin (vitamin B3), angiotensin-converting enzyme inhibitors (ACEIs), beta-blockers, and immunosuppressive drugs like cyclosporine
⇒ Now, we will discuss the clinical presentation of gout.
The clinical picture of gout

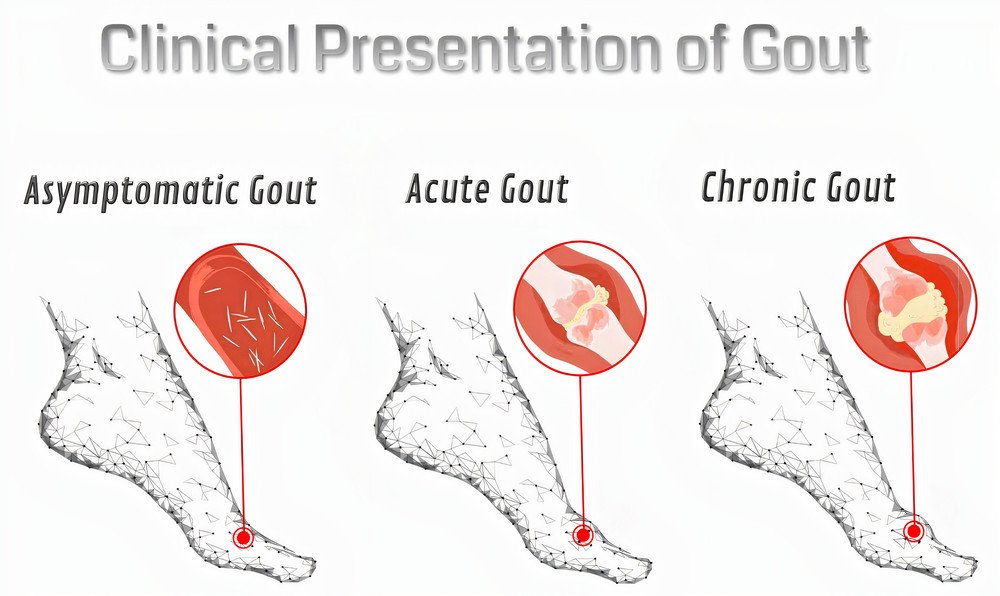
The clinical presentation of gout may be asymptomatic hyperuricemia, acute, or chronic gout. The treatment of gout will depend on the clinical presentation.
1) Asymptomatic hyperuricemia: It means just elevated levels of uric acid without pain or any other symptoms. The majority of hyperuricemic people won’t develop gout.
2) Acute gout: Acute attacks of gout show the following characters in the affected joint:
It is monoarthritis, and it usually affects the metatarsophalangeal joint of the big toe. Sometimes, it may affect the ankle, knee, dorsum of the foot, and rarely the upper limb joints.
The affected joint is painful, hot, red, tender, and with limited movement. The acute attack is so painful, and the pain usually occurs at night and reaches its maximal intensity within hours, which awakens the patient in the early morning. Fever and chills may occur during the attack. Between attacks, the patient is asymptomatic, but during recovery, some itching may occur.
The acute gout is non-erosive and resolves without deformity.
Acute gout may rarely affect multiple joints, such as in leukemia, lymphoma, longstanding gout, chronic renal failure, and post organ transplantation.
3) Chronic gout: In chronic cases, uric acid deposits in the joints (chronic gouty arthritis), kidney (gouty nephropathy), and other tissues (tophi).
- Chronic gouty arthritis shows the following features: It is polyarthritis, asymmetrical, and shows remission and exacerbation. It is erosive and causes joint deformity.
- Gouty nephropathy (urate nephropathy): The presentation of kidney affection depends on the site of uric acid deposition.
Uric acid deposition in renal tubules leads to acute renal failure. In the renal interstitial tissue, it will lead to chronic renal failure. In the urinary tract, it will cause stones, which may lead to urinary tract infections and hematuria. - Tophi: It is hard, painless, yellowish-white, gray nodules that may ulcerate and discharge gray paste material. It occurs in severe hyperuricemia and usually locates on the skin around joints, and extensor surface of the fingers, and ear lobule. It may cause permanent damage to the joint due to bone erosions.
⇒ Now, let’s discuss how your doctor will diagnose you.
Diagnosis of gout


Early diagnosis of gout is essential to avoid the chronic case, permanent damage of joints, and kidney affection. Early diagnosis also enables the doctor to differentiate between gout and other diseases that cause similar symptoms, such as septic arthritis, which is a medical emergency.
The diagnosis of gout begins with your description of the pain. If your description corresponds to the classic acute gout pain, your doctor will suspect gout. He will ask you about the previous causes and risk factors to see if the gout is secondary and to consider this in the treatment. The history may be enough for diagnosis, and the doctor may begin the treatment depending on the diagnosis with history only. But in some cases, the doctor may need further investigation to confirm his diagnosis and to exclude other conditions, such as septic (infectious) arthritis. These investigations include:
- The uric acid level in blood: In gout, it will be >7mg/dl in males and >6mg/dl in females. The average uric acid level range is (2.5 – 7) mg%. Hyperuricemia is the hallmark of gout, but it can’t exclude or confirm gout alone.
- Arthrocentesis (Synovial fluid aspiration and examination): It is the most definitive diagnostic tool. A trained physician will remove some synovial fluid from the inflamed joint and examine it under a polarized light microscope. In gout, synovial fluid will show:
- monosodium urate crystals (needle-shaped and strongly negative birefringent crystals)
- white blood cells (20000-50000 cell/mm3)
→ Arthrocentesis differentiates gout from other similar conditions, such as pseudogout, septic arthritis, and rheumatic arthritis.
- Imaging (x-ray): It may be normal in acute and early cases, but it is useful in chronic gout. In chronic gout, X-ray will show the erosions and deformity around the affected joint.
- Blood picture: Blood examination will reveal:
- Leukocytosis (increased white blood cells)
- High inflammation markers, such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)
- Kidney function tests and renal imaging: The doctor may want to see if there is monosodium urate deposition in the kidney to consider this in the treatment.
- The uric acid level in 24hour-urine: This test will be useful to detect if the problem is an overproduction or under excretion of uric acid, and this will guide the treatment. If the problem is overproduction, the uric acid will increase in 24hour-urine. But, if the problem is under excretion, uric acid will decrease in 24hour-urine. The average range of uric acid levels in 24hour urine is (250 – 750) mg.
After confirmation of gout, the doctor will start the treatment immediately to avoid progression to the chronic stage that may cause permanent joint damage and deformity, kidney affection, and tophi formation.
⇒ Now, let’s discuss the treatment of gout
Gout treatment


The treatment of gout depends on the clinical presentation (just hyperuricemia, acute, or chronic gout) and the severity of the condition. It also depends on the underlying cause, either overproduction or underexcretion.
1) In asymptomatic hyperuricemia:
Most of the hyperuricemic people won’t develop gout; thus, treatment is unnecessary. Only asymptomatic hyperuricemia will require treatment if there is:
- Positive family history of gout
- A uric acid level higher than 11mg/dl
- Increased uric acid in the urine to avoid the development of renal stones
2) In acute attacks of gout:


The goal of treatment, in this case, is to relieve the pain. We should use ice packs and pain killer medications, such as:
1. Non-steroidal anti-inflammatory drugs (NSAIDs): NSAIDs are the first-line medications in acute attacks of gout. We can use any of them, such as indomethacin, diclofenac, and ibuprofen. But, we should avoid aspirin; it may worsen the attack because it alters the uric acid level. NSAIDs have some side effects, such as peptic ulcer, salt and water retention, induction of bronchial asthma, skin rash, and nephrotoxicity. Thus, doctors may avoid them in patients with some problems, such as hypertension, heart failure, renal failure, bronchial asthma, and peptic ulcer. In patients with gastric problems, the doctors should describe proton pump inhibitors, such as omeprazole, with the NSAIDs to protect the stomach. Also, the doctors should avoid prolonged use of NSAIDS as possible (no longer than 2 or 3 days), the combination of more than one of them, and overpass the therapeutic dose.
2. Colchicine: It is a medication that relieves gout pain. It decreases the swelling around the affected joint and decreases the synthesis and deposition of uric acid crystals in the joint. It is useful for those who can’t tolerate NSAIDs due to any cause, such as hypertension, bronchial asthma, or peptic ulcer. Colchicine isn’t analgesic; thus, don’t use it in any painful condition without prescription from your doctor. It is effective at lower doses (1.2 mg for the first time, then 0.6 mg one hour later). In higher doses, some side effects may occur, such as diarrhea and vomiting. Patients with kidney failure should avoid colchicine.
3. Short term steroids: Steroids are as effective as NSAIDs, but doctors don’t prefer them due to their side effects. When the patient can’t tolerate NSAIDs or colchicine, as in renal failure, the doctor may prescribe a steroid, such as prednisone or prednisolone. But, the doctor should use the steroid at the least effective dose and for a short duration to avoid the risk of side effects.
3) In chronic gout:


In these cases, the goal of treatment is to prevent the attacks and lower the uric acid levels to the safe range. Also, in this case, we need to protect the kidney and prevent the development of stone or renal failure. In chronic gout, we may use medical treatment (hypouricemic medications) and lifestyle modifications to control the uric acid level in a better way. Medications may prevent the uric acid formation or increase their excretion. The choice depends on the underlying problem, either overproduction or underexcretion. Don’t use these hypouricemic medications until the acute attack resolves.
These medications include:
1. Allopurinol: Allopurinol inhibits the synthesis of uric acid by inhibition of the xanthine oxidase enzyme. Xanthine oxidase enzyme is essential for purine metabolism that ends with uric acid formation. It is a very cheap and effective medication. But, never use allopurinol during the acute attacks of gout because it may worsen the attack. Allopurinol may show some side effects, such as fever, diarrhea, allergy, and bone marrow depression. The dosage ranges from 100 to 300 mg/day, but the doctor should adjust the dose according to the glomerular filtration rate.
2. Febuxostat: It is also a xanthine oxidase inhibitor that decreases uric acid formation. With febuxostat, there is no need to adjust the dose based on the glomerular filtration rate. Febuxostat may show side effects, such as headache, nausea, diarrhea, arthralgia, skin rash, and elevated liver enzymes.
3. Probenecid: It is a uricosuric medication, which means that it increases the excretion of uric acid in urine. Alkalization of urine is essential with probenecid to avoid the development of renal stones. We can achieve urine alkalization by sodium or potassium citrate. The dosage of probenecid is 0.5-1gm/12hours.
4. Pegloticase: It is a new medication for the treatment of gout; it is useful in severe, treatment-resistant, and chronic cases. It converts the uric acid into allantoin, which is more soluble and easily excretable by the kidney than the uric acid. It is a recombinant procaine-like uricase. Patients take Pegloticase as an intravenous infusion every two weeks. It may cause hemolysis in patients who suffer from glucose-6-phosphate dehydrogenase deficiency.
In addition to medical treatment, your doctor will advise you to modify your lifestyle to keep uric acid within the safe range.
Lifestyle modifications


Gout occurs due to the accumulation of uric acid with large amounts, and uric acid is the product of purine metabolism. Thus, patients with gout or asymptomatic hyperuricemia should avoid purine-rich foods.
Foods-to-avoid in gout include:
- Red meat and organic meat
- Certain seafood, such as shrimp, dried anchovies, scallops, tuna, and sardines
- dried mushrooms and dried beans and peas
- poultry
Try to get other good sources of protein, such as eggs, and lean meat as chicken. Also, patients with gout should avoid refined carbohydrates, fast food, sugary drinks, and fructose-rich foods. Complex sugars may be more useful for these patients, such as fruits, vegetables, nuts, and whole grains. Also, it is better to avoid saturated fats in your diet. Low-fat dairy products help in the reduction of the gout risk. It is also useful to keep your diet plant-based.
Some recent studies have shown a beneficial effect for coffee in the reduction of uric acid levels and the risk of gout flares. Also, your doctor may prescribe vitamin-C supplements.
Alcohol is a potent risk factor for gout; thus, any patient with gout or hyperuricemia should avoid alcohol, especially beer and liquor. Excessive fluid intake (2-3 liters/day) and urine alkalization help in the protection of the kidney.
Obesity increases the risk of gout; thus, the doctor should refer obese patients who suffer from gout to a nutritionist to start a weight-reduction plan. Also, you should follow the management plan for any co-existing disease, such as hypertension and diabetes mellitus, because these diseases raise the risk of gout flares.
The target uric acid is less than 6mg/dl and, in severe cases, less than 5mg/dl.
Surgery in gout


The treatment of gout is mainly medical, and the role of surgery is limited to certain few conditions. Prolonged gout may lead to permanent damage to the affected joint and tophi. According to the situation, your doctor may recommend surgery for you. In case of extensive joint damage, your doctor may prescribe a joint replacement surgery for you. Also, your doctor may recommend the removal of tophi by surgical operation.
Also, in chronic gout, your doctor may do joint aspiration or intraarticular injection of steroids to prevent joint fibrosis and deformity.
Prognosis of gout


Gout is a chronic disease that may lead to deformity and disability if left untreated. Also, without treatment, acute attacks will be more frequent and disabling. Highly effective treatments are available. Gout has a good prognosis, with an adequate response to the therapy in most patients. Early treatment of gout and lifestyle modification lowers the risk of permanent damage and other complication, such as kidney affection or tophi formation.