

Achondroplasia is a sort of short-limbed dwarfism, which means short stature. Dwarfism divides into two types:
- Disproportionate dwarfism: average-size trunk and shorter arms and legs or a reduced trunk with longer limbs.
- Proportionate dwarfism: the body parts are in balance but shortened.
Achondroplasia is the most common form of disproportionate dwarfism. Achondroplasia means no cartilage formation. Cartilage is a firm and flexible tissue that builds up most of the skeleton during childhood in the ossification process, which means converting cartilage into bone. In achondroplasia, ossification disturbs, so the cartilage can’t grow into a complete bone, and this affects mainly the long bones of the arms and legs.
The features of achondroplasia are much severe compared to a different skeleton disorder called hypochondroplasia.
Achondroplasia affects 1 in 15,000 to 40,000 newborns. It affects males and females equally. This disorder begins during fetal life, causing skeletal dysplasia resulting in dwarfism.
Characteristic features of achondroplasia include:
- normal-sized trunk
- short arms and legs
- limitation of the elbow’s movement
- macrocephaly, which means enlarged head with a protruding forehead
Also, we find small fingers, and you may see the middle finger diverge with the ring finger giving a three-pronged (trident) appearance for the hand.
» People with achondroplasia are generally of natural intelligence.
Common health problems with achondroplasia


Recurrent ear infections, obesity, and apnea may occur. Apnea means short periods of slow and irregular breathing that may stop.
Children may suffer from abnormal curvature of the vertebral column, as follow:
- Lordosis: the sway of the lower back
- Kyphosis: abnormal front-to-back curvature of the spine
Bowed legs and back pain may also occur. Also, these infants may show delayed walking or motor skills due to decreased muscle power.
Serious complications of achondroplasia


- Spinal stenosis: It is a narrow spinal canal that may compress the upper part of the spinal cord leading to neural symptoms, such as pain, tingling, and weakness in the legs that may affect walking.
- Hydrocephalus: It is an accumulation of fluid in the brain in affected children, which leads to increased head size, several brain abnormalities that affect the motor activities of the affected child.
⇒ Now, let’s discuss achondroplasia in more detail.
Achondroplasia causes

Achondroplasia is a genetic disease that results from a mutation in the fibroblast growth factor receptor 3 (FGFR3) gene. The FGFR3 gene is responsible for the formation of a protein required for bone and brain tissue development. Normal fibroblast growth factor receptor 3 reduces the rate of bone growth. Genetic mutations make the FGFR3 protein overactive opposing skeletal development and leading to bone growth disturbances. Cartilage cannot fully develop into complete bone.
The inheritance pattern of achondroplasia


Achondroplasia is an autosomal dominant disease. An autosomal dominant design means one copy of the mutated gene per cell is enough to express the disorder. About 80 percent of people with achondroplasia have healthy parents; these cases result from new mutations in the FGFR3 gene.
In rare cases, people with achondroplasia have received an altered FGFR3 gene from one or two affected parents. People who received two mutated copies of this gene complain a critical kind of achondroplasia that causes acute shortening of the bones and an undeveloped rib cage, which is incompatible with life. These individuals are usually stillborn or die shortly after birth due to respiratory failure.
The clinical picture of achondroplasia


The main feature in people with achondroplasia is their short stature (usually under 4 feet, 6 inches) due to short arms and legs.
You can see also in these people:
- Macrocephaly (large head) with frontal bossing (forehead protruding)
- Depressed nasal bridge
- Abdomen and buttocks protrude due to the inward curvature of the vertebral column
- The vertebral column shows curvatures, either kyphosis or lordosis.
- Spinal stenosis: Narrowing of the vertebral column
- You can see tiny hands that may show a “trident” or three-pronged position when extended due to the diversion between the ring and the middle fingers.
- Reduced arms and legs (notably the upper arm and thigh)
- Bowed legs
- Decreased muscle tone, which affects the motor power of the patient
In infants, we may see the following:
- Infants with achondroplasia may have a “dome-like” (vaulted) skull with a prominent forehead.
- We may find an excessive accumulation of fluid around the brain (hydrocephalus), but it is uncommon.
- We may observe Low muscle tone (hypotonia) and delayed developmental motor functions in these affected infants.
Life expectations in achondroplasia


Numerous people with achondroplasia enjoy a natural life outlook with no difficulties. However, mortality studies have shown an increased risk for death among infants and kids under two years due to craniocervical junction abnormalities.
Achondroplasia in Children


As mentioned above, achondroplasia is a sort of short-limbed dwarfism, and it is the most popular one. An affected boy will reach a medium adult height of about 4 feet, 4 inches (52 inches), while an affected girl will reach a medium adult height of about 4 feet, 1 inch (49 inches).
Also, people with achondroplasia have natural intelligence and a natural lifespan.
Causes
Achondroplasia is a genetic autosomal dominant disease, so only one abnormal gene received from one parent leads to the case.
Most cases are the outcome of new gene mutation in families, although the parents are average height and do not have a foreign gene. Having a parent with achondroplasia enhances the risk of having many cases with this disorder. Most babies with achondroplasia do not have a family history of it.
Signs of achondroplasia in children

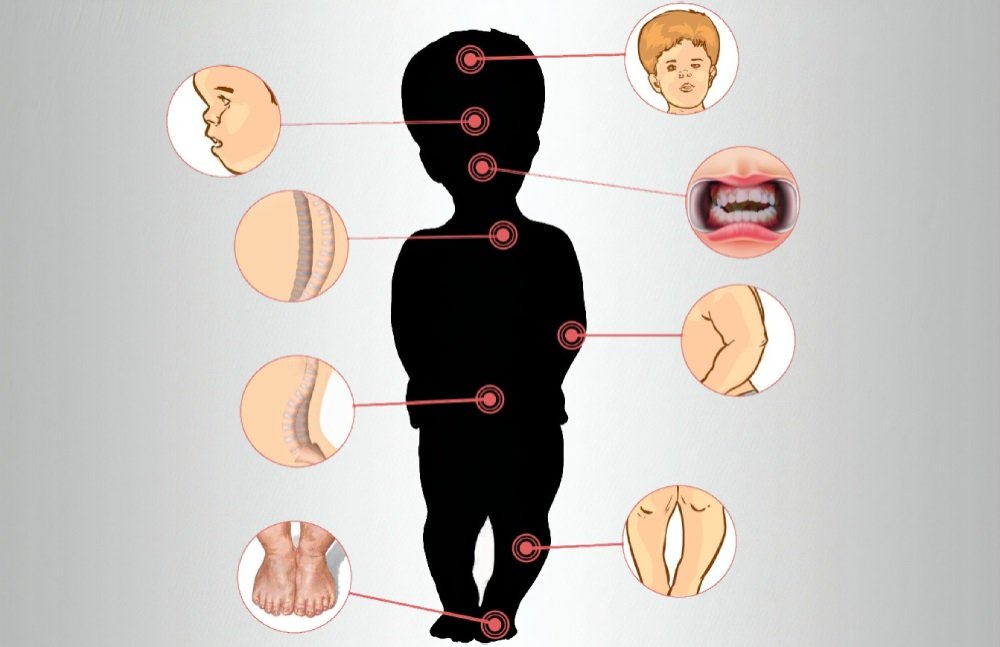
- Large size head with a broad forehead
- Flat nasal bridge
- Crowded or crooked teeth
- Short extremities, but a normal-sized trunk
- Bowed lower legs
- Curved lower spine (lordosis or sway-back), which may result in hunchback (kyphosis)
- A little hump near the shoulders that goes away after a child begins walking
- Flat feet are short and broad
Diagnosis in children


Fetal ultrasound can diagnose achondroplasia before birth. This test uses sound waves and a computer to form images of the baby growing within the womb. Fetal ultrasound may show signs of achondroplasia, such as large head and short extremities. Also, it can show the trident hand contour during fingers complete extension. We can do DNA testing before birth to confirm fetal ultrasound results.
The physical check can diagnose neonates. You have to follow your kid’s growth for any evidence of abnormal patterns and note if it’s distinctive from how your other kids grew.
Treatment in children

No treatment can reverse the condition. But, doctors have multiple options to relieve problems caused by this disease.
Surgery may be useful in correction of:
- Extra space between the middle and the ring fingers (trident hand)
- Reduced muscle tone and flaccid joints
- Short intervals of heavy or interrupted breathing (apnea)
- Hearing loss caused by Middle ear dysfunction
- Delayed developmental events, like walking happening at 18 to 24 months instead of at 12 months.
- Small canals within the spinal bones that can cause breathing problems
- Kyphosis
- Short and bowed legs
Treatment with growth hormone neither lead to natural growth nor increase the height of a person with achondroplasia.
Possible complications of achondroplasia in children


Individuals with achondroplasia show a lot of health problems, but these problems don’t occur in every child. Your child’s healthcare provider can address any of these obstacles.
Problems may include:
- Dental problems: An orthodontist should examine the child to exclude and treat any abnormal findings, such as twisted teeth. The orthodontist is a dentist who repairs the alignment of teeth.
- Ear infections: It is necessary to treat any ear infection during childhood to avoid hearing loss. Doctors can treat recurrent ear infections with ear tubes.
- We should perform check-ups for bones to control any problem, such as leg pain.
- We need to examine the spine to control any breathing problem that may happen due to the compression of the upper end of the spine. In exceptional cases, compression of the upper part of the spinal cord occurs in infancy and leads to sudden death during sleep.
- Patient with apnea suffers from difficult breathing for short periods, and infants may have episodes of apnea. Doctors can apply Surgery to remove the enlarged tonsils and adenoids to correct this problem.
- Doctors can treat regular ear infections with ear tubes.
- Hydrocephalus means an accumulation of fluid inside the brain. Doctors must drain this overloaded fluid to avoid brain affection by the insertion of a tube called a shunt.
- Posture problems: Infants may have a tiny bunch in the upper back (kyphosis). This feature disappears when a kid starts to walk. But walking results in inward curvature of the lower back (lordosis). Physical therapy may help with this problem.
- Obesity may appear and raise the risk of various diseases later in life; thus, you must follow your doctor’s guidance about ideas to keep your child’s weight healthy.
- A diseased child may have narrow vertebral canals, which are the spaces inside the spinal bones that contain the spinal cord. These narrow canals may lead to spinal cord compression as a child gets older.
Prevention in children

Most cases occur in families without a previous history, and we can’t prevent this because it is a new mutation. If one or both parents have achondroplasia, a genetic guide can provide you with data about the possibility of getting an affected child.
Life with achondroplasia means that you will adapt to be short in a world built mostly for taller individuals and expect for possible complications and manage difficulties that may happen. A healthcare unit that deals with this condition can help you support your child’s physical and emotional needs. Groups regarding these disorders can give support and knowledge to the family and the kid.
Your child will also have special protection within the public education system. You will become your child’s most valuable supporter in the school system.
Alarming signs in children to have healthcare
- Back pain
- Tingling or weakness within the arms or legs
Diagnosis of achondroplasia


Achondroplasia has clinical and radiological characteristic features. We do not require molecular testing to verify the diagnosis in many cases. When clinical features appear in a newborn, we can use X-ray (radiography) findings to verify the diagnosis. However, if there is no confirmed identification of the genetic modification of the FGFR3 gene by molecular genetics, we can use examination and imaging techniques to establish the diagnosis.
A) Clinical signs that may help in the diagnosis of achondroplasia include:
- Disproportionate short stature
- Macrocephaly with frontal bossing
- Backward displacement of the midface and flat nasal bridge
- Shortening of the arms with unnecessary skin folds covering limbs
- Limitation of elbow extension
- Shortened fingers and toes (brachydactyly)
- Trident configuration of the hands
- Bowlegs
- The excessive inward curvature of the spine (lumbar lordosis)
- Joint flaccidity
B) Radiological findings include:

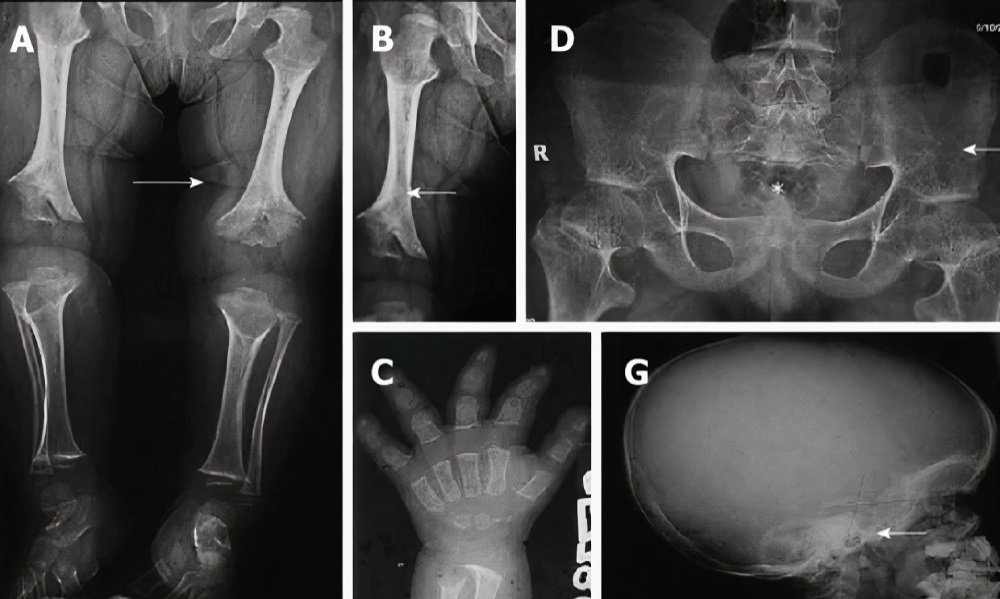
- Short ribs with cupped anterior points
- Broad hand with short metacarpals and phalanges, and a trident position
- Fibular overgrowth
- Short and dense tubular bones with metaphyseal cupping, flaring, and irregular growth services
- Small and squared iliac wings with a narrow sciatic notch and parallel acetabular roof
- Congenital narrowing of the spinal canal (spinal stenosis)
- Short and depressed vertebral bodies with nearly large intervertebral disk height
- Broad skull with a narrow foramen magnum and comparatively diminutive skull base
A skeletal overlook is valuable to confirm the diagnosis of achondroplasia.
Standard Therapies


In achondroplasia, the main goal of treatment is the correction of deformities as possible and avoid serious complications.
1) Hydrocephalus:
If signs/symptoms of increased intracranial pressure occur (such as accelerated head growth, bulging fontanelle, vision changes, headache), your doctor will refer your child to a neurosurgeon. The surgeon will do a shunt surgery to relieve the pressure on the brain.
2) Constriction of the craniocervical junction:
Medical experts should evaluate the need for suboccipital decompression because it is a hard surgery with many side effects. Indication of symptomatic compression requires urgent referral to a neurosurgeon.
3) Obstructive sleep apnea:
We can treat it with weight reduction and surgical removal of the enlarged tonsils and adenoids (adenotonsillectomy). We can apply positive airway pressure, and Surgery to create an opening in the neck (tracheostomy), but it is a rare intervention.
4) Middle ear dysfunction:
We may apply ear tubes until the age of seven or eight to manage frequent middle ear infections and prevent potential hearing loss.
5) Short stature:
Studies on the effectiveness of growth hormone have shown initial acceleration of growth, but with reducing effect over time and limited lasting benefit.
6) Obesity:
Measures to avoid obesity should begin in early infancy. We should use Standard weight-by-height grids marked for achondroplasia to monitor progress.
7) Varus deformity:
Significant bowing of the legs (Varus deformity) needs a referral to an orthopedist. However, asymptomatic bowing does not warrant surgical correction.
8) Spinal deformities:
We can apply the preventive measures that include the prohibition of unsupported sitting within the first 12-18 months of life decrease the chance of developing a set backward curve within the mid-spine (kyphosis). Doctors can apply Bracing or resort to surgical procedures, depending on the degree of hardness of such a deformity and if preventive measures failed.
9) Spinal stenosis:
If signs/symptoms of spinal stenosis occur, an urgent surgical referral is acceptable.
10) Immunization:
Routine immunizations are essential to avoid any infections that may worsen the condition and affect growth and development.
11) Adaptive needs:
Environmental adjustments of the surroundings, home, and school may be required to adapt with short stature.
12) Socialization:
Patients with achondroplasia may face challenges in socialization and school adaptation. Support groups regarding these problems can help assist families with these issues throughout peer support, personal example, and social awareness programs.